ORIGINAL LINK
“Vaccine refusal will come at a cost — for all of us,” Edward-Isaac Dovere, a staff writer for The Atlantic, proclaims in an April 10, 2021, political commentary.1 Unvaccinated individuals “will have higher health care costs,” he says, and the vaccinated will have to foot the bill, either through taxes or insurance premiums.
This argument could have been made for decades, and can still be made today, for any number of groups. Obese individuals have far higher health care costs than those of normal weight. Insulin resistant people and those with Type 2 diabetes end up costing the health care system enormous sums. Who pays for them?
Overall, healthy individuals — people who generally do what they can to take good care of themselves to prevent chronic conditions — have always paid for those who are less particular about their diets and lifestyle.
The Economic Costs of Vaccination Vs. Vaccine Refusal
Dovere predicts the economic costs of vaccine refusal will begin to feature heavily as we move forward. He quotes Washington Gov. Jay Inslee, who told him,2 “You have a liberty right, and that unfortunately is imposing on everyone else and their liberty right not to have to pay for your stubbornness.” Not surprisingly, Dovere and Inslee both focus on just one side of what needs to be a two- if not four-sided equation.
When making public health policy, you have an obligation to analyze both the benefit and the cost of any given policy. In this case, what might be the cost of vaccine side effects, both in terms of health care costs and lives lost? As of April 1, 2021, VAERS had received 56,869 adverse events following COVID-19 vaccination, including 7,971 serious injuries and 2,342 deaths.3 By April 13, the had updated that death toll to 3,005.4
What might be the cost if the vaccines don’t work and you get sick anyway? As of April 15, 2021, some 5,800 Americans who had been fully vaccinated against COVID-19 had been diagnosed with COVID-19 post-vaccination; 396 (7%) required hospitalization and 74 died.5 These cases are popping up all over the world.
The vaccines are not foolproof. In fact, so-called “breakthrough cases,” meaning cases in which a fully vaccinated individual is diagnosed with COVID-19 are to be expected. I’m not sure why anyone is surprised, seeing how the vaccine makers have acknowledged that the mRNA injections are not designed to actually make you immune to SARS-CoV-2.
You can still contract the virus and spread it to others. What the shots may do is lessen your symptoms if and when you get infected with SARS-CoV-2. So, of course people can still get sick, as they did before. Some will require hospitalization. Some will die — just like they did previously, before the vaccine.
Then there’s the question of whether vaccinated individuals end up being more susceptible to variants of the virus than unvaccinated individuals. Preliminary research6,7,8,9 found that people who had received both doses of the Pfizer COVID-19 vaccine were eight times more susceptible to contracting the South African variant of SARS-CoV-2, called B.1.351, (5.4% compared to 0.7%).
Unfortunately, the study was too small to glean any information about outcomes, so we don’t know whether they developed milder or more serious illness than unvaccinated people sickened by the same variant.
Either way, if vaccinated people are more susceptible to more dangerous variants (which they claim B.1351 is), why assume that unvaccinated people would incur higher health care costs? Variants are now cropping up all over the place, so maybe vaccinated people will end up being responsible for a greater share of medical expenses. Maybe, if they have milder illness and unvaccinated have more serious illness, the costs might end up about the same for each group.
May There Be Economic Benefits to Vaccine Refusal?
In my view, the notion that COVID-19 vaccines will end this pandemic is an illogical fallacy since these shots do not provide actual immunity. The fizz in Dovere’s argument starts going flat on that basis alone. But there’s much more.
To really determine what’s best for public health, you’d also want to do the benefit and cost analysis of not vaccinating and relying on naturally-acquired immunity in combination with immune-boosting strategies instead, such as improving vitamin D levels across the entire population, for example.
Only when you have made all of those calculations — the benefit and cost of vaccinating, and the benefit and cost of not vaccinating — can you compare the two and begin to make statements about how certain groups of people may incur higher health care costs, and which strategy is likely to save the most lives. As of right now, it’s pure guesswork as to who’s going to cost more in the long run.
For example, I don’t know of any actual data showing that the health of people who are planning to forgo the vaccine place them at increased risk of serious COVID-19. If I were to guess, and this is pure speculation, people who have decided not to get vaccinated may be doing so because a) they know they’re in a low-risk category and/or b) they are health-conscious people who feel confident that they can prevent and/or treat COVID-19 in other cost-effective ways, should they get sick.
There are a lot of data that need to be compiled and analyzed before we can start declaring the COVID-19 vaccination campaign a public health care success, let alone a cost-saving imperative.
Appeal to Illogical Reasoning
Dovere goes on to discuss some of the messaging campaigns employed to lure people out of their vaccine hesitancy:10
“Two appeals seem to work best: First, the vaccines are safe, and they’re more effective than the flu vaccine. Second, you deserve this, and getting vaccinated will help preserve your liberty and encourage the government to lift restrictions.
(That last idea is what Jerry Falwell Jr. focused on in the vaccination selfie he posted11 this week, captioned, ‘Please get vaccinated so our nutcase of a governor will have less reasons for mindless restrictions!’) Inslee hopes that emphasizing those points will persuade more Republican men to get their shots.”
Sometimes it can help to spell out a logical fallacy using different words. (Personally, I believe Falwell was simply trying to be funny, but Dovere and Inslee have apparently seized the “lift restrictions” angle as a social conditioning opportunity, so that’s really what I’m addressing here.)
One rewrite of Falwell’s plea could be: “Please ignore your current health status and potential vaccine risks and just obey so that our governor will have less reason to impose unconstitutional and unscientific limitations on our basic rights and freedoms.”
In my view, a more appropriate way to prevent “mindless restrictions” would be to peacefully disobey and/or take the governor to court, as has been done to California Gov. Gavin Newsom. The Supreme Court has ruled against him no less than six times, finding he abused his power, overstepped his authority and violated the Constitution with his pandemic restrictions on churches.12
Urging someone to take a vaccine to prevent an elected official — who can be unseated — from implementing unscientific and/or unconstitutional restrictions is hardly rational. Let’s not forget that cost-benefit analyses13 have actually been done for lockdowns — perhaps one of the most mindless of restrictions — and the cost is far greater than the benefit.
The cost of the lockdowns in the U.K., in terms of Wellbeing Years (WELLBY), is five times greater than might optimistically be saved, and may in reality be anywhere from 50 times to 87 times greater. The cost for lockdowns in Canada is at least 10 times greater than the benefit.
In Australia, the minimum cost is 6.6 times higher, and in the U.S., the cost is estimated to be at least 5.2 times higher than the benefit of lockdowns. A cost-benefit analysis performed for New Zealand, which looked at the cost of adding just five extra days of “COVID-19 alert level 4” found the cost in Quality Adjusted Life Years (QALY) was 94.9 times higher than the benefit.
Should We Penalize Obesity and Vitamin D Deficiency?
If it’s determined that unvaccinated individuals need to be penalized socially, financially or otherwise, then how can we not also penalize other choices that significantly add to the COVID-19 burden? We know, for example, that vitamin D deficiency significantly raises your risk of COVID-19. In one analysis,14 82.2% of COVID-19 patients were vitamin D deficient.
I published a scientific review15 on the impact of vitamin D in COVID-19 in October 2020, co-written with William Grant, Ph.D., and Dr. Carol Wagner, both of whom are part of the GrassrootsHealth expert vitamin D panel. You can read the paper for free on the journal’s website.
Another major COVID-19 factor is obesity. As reported by CNN16 March 5, 2021, the COVID-19 death rates were more than 10 times higher in countries where more than half the adult population was overweight, compared to countries in which the obesity rate was below 50%. The COVID-19 death rates also rose in tandem with the prevalence of obesity, thereby strengthening the link, according to the report, released by the World Obesity Federation.
At the lowest end is Vietnam, which has an obesity rate of 18.3% and a COVID-19 death rate of 0.04 per 100,000. Toward the high end is the U.S., which has an obesity rate of 67.9% and a COVID-19 death rate of 152.49 per 100,000. (Of course, this report used COVID-19 mortality statistics that have been proven to be wildly exaggerated, as detailed in my interview with Dr. Henele.)
Making an already dire situation worse, recent data17 show 42% of U.S. adults have packed on unwanted pounds, with an average weight gain of 29 pounds, since the start of the pandemic. Only 18% report undesired weight loss, with an average weight loss of 26 pounds.
Government Has Ignored the Value of Healthy Population
According to the World Obesity Federation report, obesity was the second most important risk factor for hospitalization and death from COVID-19 — old age being the primary risk factor — and as noted by Johanna Ralston, CEO of the World Obesity Federation:18
“Old age is unavoidable, but the conditions that contribute to overweight and obesity can be highly avoidable if governments step up and we all join forces to reduce the impact of this disease. The failure to address the root causes of obesity over many decades is clearly responsible for hundreds of thousands of preventable deaths."
Lead author of the report, Dr. Tim Lobstein, added:19
"Governments have been negligent, and ignored the economic value of a healthy population at their peril. For the last decade they have failed to tackle obesity, despite setting themselves targets at United Nations meetings. COVID-19 is only the latest infection exacerbated by weight issues, but the warning signs were there. We have seen it in the past with MERS, H1N1 and other respiratory diseases.”
Let’s Not Accept Hypocrisy and Double Standards
Even WHO Director-General Tedros Adhanom Ghebreyesus commented on the report saying it “must act as a wake-up call to governments globally,” as "The correlation between obesity and mortality rates from COVID-19 is clear and compelling."
That said, let’s get back to Dovere’s argument that unvaccinated people are bound to incur higher health care costs due to COVID-19, and therefore there must be some way to penalize those people or force them into compliance.
If you cannot fathom penalizing obesity, insulin resistance, diabetes or vitamin D deficiency — conditions known to significantly raise your risk of severe COVID-19 — then how could you possibly consider penalizing an unvaccinated person based on that single parameter alone?
Using that logic, what, then, do we need to do about obese individuals, whose risk of hospitalization due to COVID-19 is anywhere from 40% to 113% greater, and their chances of requiring intensive care 74% higher,20 than that of their non-obese peers? What do we need to do about people who just refuse to get their vitamin D levels up, and end up taking up the lion’s share of hospital beds?
To be clear, I am NOT proposing we penalize people based on their weight, metabolic flexibility or vitamin D status. I do not support that any more than I support penalizing unvaccinated people — and that is the whole point. Most would agree that this would be completely ridiculous.
My point is, if you cannot fathom penalizing obesity, insulin resistance, diabetes or vitamin D deficiency — conditions known to significantly raise your risk of severe COVID-19 — then how could you possibly consider penalizing an unvaccinated person based on that single parameter alone?
The question is especially valid because, again, vaccinated persons can contract and spread SARS-CoV-2 like anyone else. It’s really unclear how vaccinated people are “safer” than unvaccinated ones, when the only person standing to gain from these shots is the person getting it (in the form of milder symptoms when sickened).
Are You ‘Pure’ Enough for Your Government?
I think it’s important to realize that the COVID-19 vaccine campaign is less about protecting public health and more about creating the infrastructure and psychological climate required for the implementation of global tyranny, which will likely begin with the introduction of vaccine passports that are very similar to the China social credit system.
As discussed in “Vaccines Are the New ‘Purity Test,’” it can almost be likened to a loyalty test. Or perhaps it could best be described as a totalitarian submission test?
Getting private companies to require these vaccine passports only makes sense if there is a strong vaccine push, and this is one of many clues as to what’s really behind the stated “need” for the whole world to get vaccinated.
We’re not all at risk for COVID-19. For a vast majority of individuals, the vaccines make little or no sense, as for young, healthy individuals, their risks outweigh the benefit. Now they are pushing to vaccinate children, whose risk of getting COVID-19 is well-established as being profoundly minuscule.
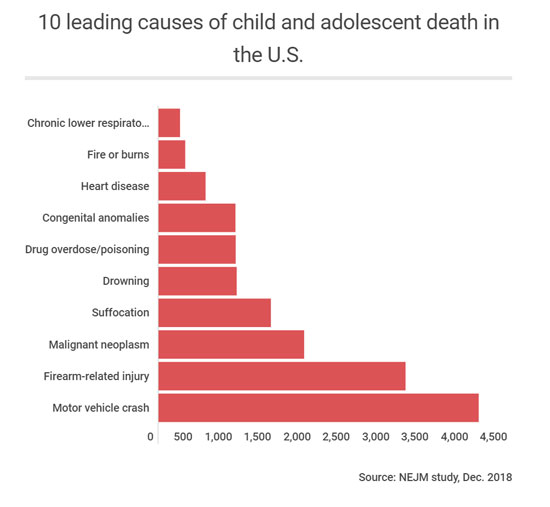
They are at exponentially higher risk from many other factors. There are currently fewer than 500 children who are reported to have died from COVID-19, even with the massively manipulated causes of death. Remember, if you had a positive COVID test and died from terminal cancer or a motorcycle accident, you were classified as a COVID-19 death.
As you can see from the graph below, there are 10 higher risks of death than COVID-19 for children. To be logically consistent, the government would need to be equally rigid about addressing all of these causes as aggressively as they are pursuing COVID-19 vaccination for children.
But it’s not about simply getting a vaccine into your arm. Ultimately, it’s about getting you tied into the digital system being launched in the form of vaccine passports. As explained by former Clinton adviser and author Naomi Wolf (whom I will be interviewing shortly) in a March 28, 2021, interview with Fox News’ Steve Hilton:21,22
“‘Vaccine passport’ sounds like a fine thing if you don’t understand what those platforms can do. I’m [the] CEO of a tech company, I understand what these platforms can do. It is not about the vaccine, it’s not about the virus, it’s about your data.
Once this rolls out, you don’t have a choice about being part of the system. What people have to understand is that any other functionality can be loaded onto that platform with no problem at all. It can be merged with your Paypal account, with your digital currency. Microsoft is already talking about merging it with payment plans.
Your network can be sucked up. It geolocates you everywhere you go. You credit history can be included. All of your medical and health history can be included … It is absolutely so much more than a vaccine pass … I cannot stress enough that it has the power to turn off your life, or to turn on your life, to let you engage in society or be marginalized.”
Dangerous Curves Ahead
Wolf also points out the horrific history of IBM, which developed a sophisticated system of punch cards that allowed Nazi Germany to create a two-tier society and ultimately facilitated the rounding up of Jews for extermination. Fast-forward to today, and IBM is now a leader in the vaccine passport business. I wrote about this in “IBM Colluded With Hitler, Now Makes Vaccine Passports.”
In Nazi Germany, the obsession with purity — both in terms of hygiene and race theory — drove the genocide of Jews, the old, the handicapped and the mentally challenged.
In present day, the public narrative has eerily followed Nazi Germany’s playbook for genocide, starting with the scapegoating of healthy people, as the rapid spread of COVID-19 was blamed on asymptomatic individuals not properly masking, social distancing and self-isolating.
That then grew into the nurturing of prejudice against people who refuse to wear masks, and now we’re seeing the narrative building toward persecution of those who do not want to get the vaccine. It will start with discrimination, and already, we’re hearing talk of how only vaccinated people ought to have the right to partake in certain social activities. If that is tolerated, then outright persecution will be the inevitable next step.
This is why I reject and counter commentaries such as that by Dovere. These half-baked, one-sided, persecutory arguments must be challenged at every turn, because they only lead us one way. And unless you’re part of the technocratic elite, you — regardless of how you feel about vaccination right now — do not want to end up there.

via
IFTTT
InoreaderURL:
SECONDARY LINK

















{kind=link}
{kind=link}