
The oft-repeated refrain right now is that we’re in a “pandemic of the unvaccinated,” meaning those who have not received the COVID jab make up the bulk of those hospitalized and dying from the Delta variant. For example, August 20, 2021, England’s chief medical officer professor Chris Whitty tweeted:1,2
“Four weeks working on a COVID ward makes stark the reality that the majority of our hospitalized COVID patients are unvaccinated and regret delaying. Some are very sick including young adults. Please don’t delay your vaccine.”
Curiously, if you take the time to actually look at the data, you’ll find that this blanket statement is rather deceptive. Here’s a graphic published in the Evening Standard, sourced from Public Health England:3
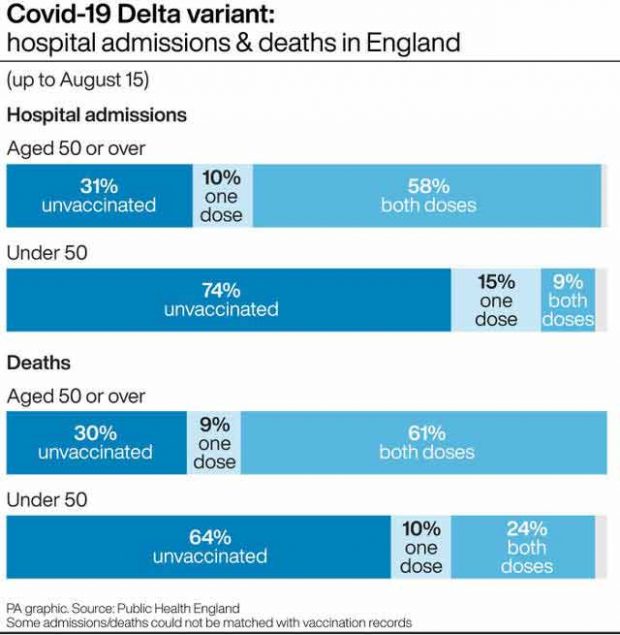
As you can see, as of August 15, 2021, 58% of COVID patients admitted to hospital who were over the age of 50 had actually received two doses of COVID injections and 10% had received one dose. So, partially or fully “vaccinated” individuals made up 68% of hospitalizations.
Only in the 50 and younger category were a majority, 74%, of hospitalizations among the unvaccinated. Whitty, however, completely neglected to differentiate between the age groups. The same applies to deaths. Unvaccinated only make up the majority of COVID deaths in the under-50 age group. In the over-50 group, the clear majority, 70%, are either partially or fully “vaccinated.”
It’s also unclear whether hospitals in the U.K. (and elsewhere) are still designating anyone who is admitted and tests positive with a PCR test as a “COVID patient.” If so, people with broken bones or any number of other health problems who have no symptoms of COVID-19 at all might be unfairly lumped into the “unvaccinated COVID patient” total.
Israeli Data Show COVID Jab Is Failing in Over-50s
In Israel, where vaccine uptake has been very high due to restrictions on freedom for those who don’t comply,4 data show those who have received the COVID jab are 6.72 times more likely to get infected than people with natural immunity.5,6,7
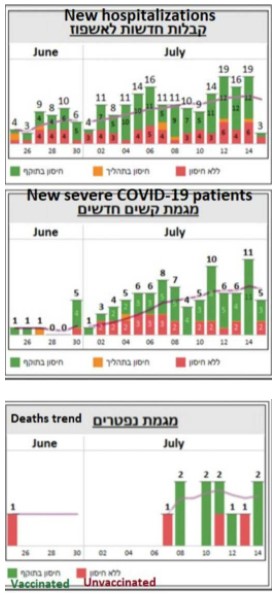
The fully “vaccinated” also made up the bulk of serious cases and COVID-related deaths in July 2021, as illustrated in the graphs below.8 The red is unvaccinated, yellow refers to partially “vaccinated” and green fully “vaccinated” with two doses. By mid-August, 59% of serious cases were among those who had received two COVID injections,9 mirroring the data coming out of the U.K.
In an August 16, 2021, Science article,10 Israeli Minister of Health Nitzan Horowitz is quoted saying the nation has entered a “critical time” in the race against the pandemic. Horowitz allegedly was given a third booster shot August 13, 2021, the day they began offering a third dose to people over the age of 50.
From Public Health England’s data, it seems clear that the COVID shots are failing to protect people over the age of 50 in the U.K. as well, so it’s probably only a matter of time before booster shots are rolled out there too. And, provided the COVID injections are the same irrespective of country, there’s every reason to assume the same trends will emerge in other countries, including the U.S.
This is precisely what Ran Balicer, chief innovation officer at Clalit Health Services, Israel’s largest health maintenance organization (HMO), told Science: “If it can happen here, it can probably happen everywhere.”11
Israeli Data Considered the Best Around
The data coming out of Israel is considered by many to be the best we have, and can give us a glimpse of what to expect elsewhere. As explained by Science magazine:12
“Israel is being closely watched now because it was one of the first countries out of the gate with vaccinations in December 2020 and quickly achieved a degree of population coverage that was the envy of other nations — for a time.
The nation of 9.3 million also has a robust public health infrastructure and a population wholly enrolled in HMOs that track them closely, allowing it to produce high-quality, real-world data on how well vaccines are working.
‘I watch [Israeli data] very, very closely because it is some of the absolutely best data coming out anywhere in the world,’ says David O’Connor, a viral sequencing expert at the University of Wisconsin, Madison.
‘Israel is the model,’ agrees Eric Topol, a physician-scientist at Scripps Research. ‘It’s pure mRNA vaccines. It’s out there early. It’s got a very high level population [uptake]. It’s a working experimental lab for us to learn from.’
Israel’s HMOs … track demographics, comorbidities, and a trove of coronavirus metrics on infections, illnesses, and deaths. ‘We have rich individual-level data that allows us to provide real-world evidence in near–real time,’ Balicer says …
Now, the effects of waning immunity may be beginning to show in Israelis vaccinated in early winter; a preprint13 published last month … found that protection from COVID-19 infection during June and July dropped in proportion to the length of time since an individual was vaccinated.People vaccinated in January had a 2.26 times greater risk for a breakthrough infection than those vaccinated in April.”
Where Will It End?
According to Science magazine, breakthrough cases are now multiplying at breakneck speed. “There are so many breakthrough infections that they dominate and most of the hospitalized patients are actually vaccinated,” Uri Shalit, a bioinformatician at the Israel Institute of Technology told Science.14
Nearly 1 million Israelis over the age of 50 have now received a third booster of Pfizer’s mRNA shot. Time will tell whether this will worsen the rate of breakthrough cases or tame it.
Dvir Aran, a biomedical data scientist at the Israel Institute of Technology doesn’t seem very hopeful, telling Science the surge is already so steep, “even if you get two-thirds of those 60-plus [boosted], it’s just gonna give us another week, maybe two weeks until our hospitals are flooded” again.15
The obvious question is, what then?! Will the answer be a fourth injection before the year is over? Will we be looking at quarterly injections? Monthly injections? Biweekly? Weekly? Where and when does it end? It is fairly easy to predict that this can only end very badly.
US Tracks Only Fraction of Breakthrough Infections
Unfortunately, we cannot rely on U.S. data to get a clear idea of how the COVID shots are working, as the U.S. Centers for Disease Control and Prevention has chosen not to track all breakthrough cases. As reported by ProPublica,16 May 1, 2021, the CDC stopped tracking and reporting all breakthrough cases, opting to log only those that result in hospitalization and/or death.
As noted in the article, this irrational decision has “left the nation with a muddled understanding of COVID-19’s impact on the vaccinated.” It also prevents us from understanding how variants are spreading and whether those who have received the jab can still develop so-called “long-haul syndrome.”
Individual states are also setting their own criteria for how they collect data on breakthrough cases, and this patchwork muddies the waters even further. Despite these limitations, what little data we do have is starting to mirror that of Israel and the U.K.
August 18, 2021, the CDC released three reports,17,18,19 which show the protection you get from the COVID shot is rapidly waning.
“Among nursing home residents, one of the studies showed vaccine effectiveness dropped from 74.7% in the spring to just 53.1% by midsummer,”ProPublica writes.20 “Similarly, another report found that the overall effectiveness among vaccinated New York adults dropped from 91.7% to just under 80% between May and July.
The new findings prompted the Biden administration to announce on Wednesday that people who got a Moderna or Pfizer vaccine will be offered a booster shot eight months after their second dose. The program is scheduled to begin the week of Sept. 20 but needs approval from the Food and Drug Administration and a CDC advisory committee.
This latest development is seen by some as another example of shifting public health messaging and backpedaling that has accompanied every phase of the pandemic for 19 months through two administrations. A little more than a month ago, the CDC and the FDA released a joint statement saying that those who have been fully vaccinated ‘do not need a booster shot at this time’ …
The CDC tracked all breakthrough cases until the end of April, then abruptly stopped without making a formal announcement. A reference to the policy switch appeared on the agency’s website in May about halfway down the homepage.
‘I was shocked,’ said Dr. Leana Wen, a physician and visiting professor of health policy and management at George Washington University. ‘I have yet to hear a coherent explanation of why they stopped tracking this information’ …
Sen. Edward Markey, D-Mass., became alarmed after the Provincetown outbreak and wrote to CDC director Dr. Rochelle Walensky on July 22, questioning the decision to limit investigation of breakthrough cases. He asked what type of data was being compiled and how it would be shared publicly21 … Markey asked the agency to respond by Aug. 12. So far the senator has received no reply …”
Vaxxed Are Up to 13 Times More Likely to Get Delta Variant
While the U.S. is lax about recording breakthrough infections, researchers in Israel have some breaking news: They have been keeping track, and their studies22 show that vaccinated individuals are up to 13 times more likely to get the Delta variant of COVID-19 than those who were not vaccinated, but had recovered from a COVID infection.
As explained by ScienceMag:23 The study “found in two analyses that people who were vaccinated in January and February were, in June, July and the first half of August, six to 13 times more likely to get infected than unvaccinated people who were previously infected with the coronavirus. In one analysis, comparing more than 32,000 people in the health system, the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalization eight times higher.”
The study also said that, while vaccinated persons who also had natural infection did appear to have additional protection against the Delta variant, the vaccinated were still at a greater risk for COVID-19-related-hospitalizations compared to those without the vaccine, but who were previously infected. Vaccinees who hadn’t had a natural infection also had a 5.96-fold increased risk for breakthrough infection and a 7.13-fold increased risk for symptomatic disease.
One thing to note here is that the wording of this is important: The study does not say that getting a vaccine helps protect you if you’ve had a natural infection; rather, it says that natural protection helps boost the vaccine. Either way, even if you do have natural infection in combination with the vaccination, vaccinees are still at an increased risk for a breakthrough infection.
“This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity,” the study authors concluded.
Fully Vaxxed Speak Out
Back America, in an August 24, 2021, article,24 The Defender cites data from seven states (California, Colorado, Massachusetts, Oregon, Utah, Vermont and Virginia) that keep more detailed records than most. In six of these states, breakthrough infections accounted for 18% to 28% of all new COVID diagnoses in the past several weeks, as well as 12% to 24% of all COVID-related hospitalizations.
In Los Angeles, breakthrough cases have risen from 5% in April and 13% in July to a current of 30%. Fully vaxxed celebrities and elected officials have now started speaking out after getting COVID. As reported by The Defender: 25
“Melissa Joan Hart, the former ‘Sabrina the Teenage Witch’ star is ‘really mad’ she has a breakthrough case. Hart shared on Instagram Aug. 19 … ‘I got COVID. I am vaccinated. And I got COVID. And it’s bad. It’s weighing on my chest, it’s hard to breathe’ …
Celebrity Hilary Duff, revealed she had COVID on Instagram Aug. 20. Duff said she was experiencing a bad headache, brain fog, sinus pressure and a loss of taste and smell despite being vaccinated …
Slipknot singer Corey Taylor, 47, was devastated after testing positive for COVID and was forced to call off his upcoming appearance at a Michigan pop culture convention this weekend, Rolling Stone reported. ‘I wish I had better news,’ said Taylor in a recorded video message last week on Facebook. ‘I woke up today and tested positive and I’m very, very sick’ …
Rev. Jesse Jackson, and his wife, Jacqueline, remained under doctors’ observation Monday[August 23, 2021] at a Chicago hospital after getting COVID … Jackson, a Chicago civil rights leader, was fully vaccinated and received his first dose in January during a publicized event where he urged others to receive the vaccine as soon as possible …
Three U.S. senators — John Hickenlooper (D-Colo.), Angus King (I-Maine) and Roger Wicker (R-Miss.) — announced Aug. 19 they tested positive for COVID despite being fully vaccinated, CBS News reported …
The news came days after Texas Gov. Greg Abbott, who also was fully vaccinated, tested positive for COVID. Illinois state Sen. Dan McConchie announced Aug. 21 he had a ‘breakthrough’ case of COVID.”
CDC Has Also Hidden Breakthrough Cases in Other Ways
The CDC also cooked the books on COVID breakthrough cases in other ways. Originally, the CDC recommended labs use a CT of 4026 when testing for SARS-CoV-2 infection. This, despite using a CT above 35 was known to create a false positive rate of 97%.27 By using an exaggerated CT, healthy people were deemed stricken with COVID-19.
In May 2021, the CDC lowered the CT from 40 to 28 or lower — but only when doing PCR testing on individuals who have received the COVID jab.28 Unvaccinated were still tested using a CT of 40. The end result is obvious: “Vaccinated” individuals became far less likely to test positive for SARS-CoV-2 infection while unvaccinated were still exceedingly getting false positives. As noted by Off-Guardian:29
“This is a policy designed to continuously inflate one number, and systematically minimize the other. What is that if not an obvious and deliberate act of deception?”
How the CDC Invented the ‘Pandemic of Unvaxxed’ Narrative
The CDC also played fast and loose with the data when it invented the “pandemic of the unvaccinated” narrative30 that we’re now being indoctrinated with. In a July 16, 2021, White House press briefing,31 CDC director Dr. Rochelle Walensky claimed “over 97% of people who are entering the hospital right now are unvaccinated.”
Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe. ~ Dr. Bart Classen, Trends in Internal MedicineAs it turns out, that statistic is based on hospitalization data from January through June 2021, when the majority of Americans had not yet gotten the COVID jab. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,32 and as of June 30, just 46.9% were “fully vaccinated.”33
COVID Shots ‘Proven to Cause More Harm Than Good’
While the official narrative is that the COVID shots may be “less than perfect” but are still better than the alternative (i.e., getting the infection when you’re unvaccinated), Dr. Bart Classen published a study34 in the August 2021 issue of Trends in Internal Medicine, disputing this claim.
The study,35 “U.S. COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, ‘All Cause Severe Morbidity,'” details a core problem with Pfizer’s, Moderna’s and Janssen’s (Johnson & Johnson) trials.
All three employ a surrogate primary endpoint for health, namely “severe infections with COVID-19.” This, Classen says, “has been proven dangerously misleading,” and many fields of medicine have stopped using disease-specific endpoints in clinical trials and have adopted “all-cause mortality and morbidity” instead.
The reason for this is because if a person dies from the treatment or is severely injured by it, even if the treatment helped block the progression of the disease they’re being treated for, the end result is still a negative one.
To offer an extreme example of what you can do with a disease-specific endpoint, you could make the claim that shooting people in the head is a cure for cancer, because no one who got the treatment — who got shot in the head — died from cancer.
When reanalyzing the clinical trial data from these COVID shots using “all-cause severe morbidity” as the primary endpoint, the data reveal they actually cause far more harm than good.
The proper endpoint was calculated by adding together all severe events reported in the trials, not just COVID-19 but also all other serious adverse events. By doing this, severe COVID-19 infection gets the same weight as other adverse events of equivalent severity. According to Classen:36
“Results prove that none of the vaccines provide a health benefit and all pivotal trials show a statistically significant increase in ‘all cause severe morbidity’ in the vaccinated group compared to the placebo group.
The Moderna immunized group suffered 3,042 more severe events than the control group. The Pfizer data was grossly incomplete but data provided showed the vaccination group suffered 90 more severe events than the control group, when only including ‘unsolicited’ adverse events.
The Janssen immunized group suffered 264 more severe events than the control group. These findings contrast the manufacturers’ inappropriate surrogate endpoints:
Janssen claims that their vaccine prevents 6 cases of severe COVID-19 requiring medical attention out of 19,630 immunized; Pfizer claims their vaccine prevents 8 cases of severe COVID-19 out of 21,720 immunized; Moderna claims its vaccine prevents 30 cases of severe COVID-19 out of 15,210 immunized.
Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.”
To make the above numbers more clear and obvious, here are the prevention stats in percentages:
- Pfizer 0.00036%
- Moderna 0.00125%
- Janssen 0.00030%
Where Do We Go From Here?
If you’ve already gotten one or two shots, there’s nothing you can do about that. It seems pretty obvious, though, if you objectively analyze the data, that your best bet is to say no to any and all future boosters, as each additional shot can magnify the damage and increase your risk of serious side effects.
If you develop symptoms of SARS-CoV-2 infection, there are several treatment protocols available that have been shown to be effective. Options include the Zelenko protocol,37 the MATH+ protocols38 and nebulized hydrogen peroxide, as detailed in Dr. David Brownstein’s case paper39 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.”
Whichever treatment protocol you use, make sure you begin treatment as soon as possible, ideally at first onset of symptoms. Also, realize that if you’ve gotten one or more COVID shots, your risk of severe infection may actually be greater, not lesser, than had you not gotten the injections. This appears particularly true if you’re over the age of 50. So, do not delay treatment if you develop symptoms.
Sources and References
- 1 Twitter August 20,2021
- 2, 3 Evening Standard August 20, 2021
- 4 Our World in Data, Data for Israel
- 5 David Rosenberg 7 July 13, 2021
- 6 Sharylattkisson.com August 8, 2021
- 7 Sharylattkisson.com August 6, 2021
- 8 Twitter Alex Berenson July 18, 2021
- 9, 10, 11, 12, 14, 15 Science August 16, 2021
- 13 medRxiv July 31, 2021 DOI: 10.1101/2021.07.29.21261317 (PDF)
- 16, 20 ProPublica August 20, 2021
- 17 CDC MMWR August 18, 2021; 70 New COVID Cases and Hospitalizations Among Adults by Vaccination Status
- 18 CDC MMWR August 18, 2021; 70 Sustained Effectiveness of Pfizer and Moderna Vaccines Against COVID Associated Hospitalizations Among Adults
- 19 CDC MMWR August 18, 2021; 70 Effectiveness of Pfizer and Moderna Vaccines Among Nursing Home Residents
- 21 Ed Markey Press Release July 22, 2021
- 22 MedRxiv August 25, 2021
- 23 ScienceMag August 26, 2021
- 24, 25 The Defender August 24, 2021
- 26 FDA.gov CDC 2019-nCoV Real-Time RT-PCR Diagnostic Panel Instructions, July 13, 2020 (PDF) Page 35
- 27 Clinical Infectious Diseases September 28, 2020; ciaa1491
- 28, 29 Off-Guardian May 18, 2021
- 30 The New York Times July 16, 2021
- 31 WH.gov Press Briefing July 16, 2021
- 32 Bloomberg COVID Vaccine Tracker
- 33 Mayo Clinic COVID Vaccine Tracker
- 34, 35, 36 Trends in Internal Medicine August 2021; 1(1): 1-6
- 37 Zelenko protocol
- 38 Covid19criticalcare.com
- 39 Science, Public Health Policy and The Law July 2020; 1: 4-22 (PDF)
The post 60% of Those Older Than 50 Who Die From Covid Are Double Vaxxed appeared first on LewRockwell.
via IFTTT
InoreaderURL: SECONDARY LINK

